President Biden Signs End-of-Year Legislation Including Telehealth, Medicare & Medicaid, Mental Health, Pandemic Preparedness, and Other Health Care Provisions
What You Need to Know
Key takeaway #1
The Consolidated Appropriations Act, 2023 funds the federal government through fiscal year 2023, including funding for the Department of Health and Human Services and its agencies. It makes numerous health care policy changes, including on telehealth, Medicare and Medicaid programs, mental health, clinical trials diversity and modernization, and pandemic preparedness and other public health efforts.
Key takeaway #2
To advocate for priorities not addressed in the legislation, stakeholders will have opportunities in the 118th Congress to pursue policy priorities through must-pass legislation and reauthorization of programs and through the federal rulemaking process.
Client Alert | 12 min read | 01.25.23
On December 29, President Joe Biden signed into law the Consolidated Appropriations Act, 2023 (P.L. 117-164) (the “Act”)—an approximately $1.7 trillion spending package, which consists of all 12 fiscal year (FY) 2023 appropriations bills and funds the federal government through September 30, 2023, provides additional assistance to Ukraine, and makes numerous health care policy changes.
The Act includes the following health care provisions:
- Extends certain Medicare telehealth flexibilities enacted during the COVID-19 public health emergency (PHE) for two years, through December 31, 2024;
- Extends the Acute Hospital Care at Home program for two years, through December 31, 2024;
- Mitigates Medicare payment reductions to health care providers and makes other Medicare payment policy changes;
- Provides funding for numerous mental health and substance use disorder programs and implements mental health parity requirements;
- Requires private Medicaid carriers and other managed care companies to publish and regularly update directories of in-network health care providers;
- Requires state Medicaid programs to provide 12 months of continuous coverage for children and permanently allow states to offer 12 months of coverage for postpartum women;
- Requires the Food and Drug Administration (FDA) to issue guidance to improve diversity in clinical trials, advance the use of decentralized clinical trials, and review the appropriate use of digital health technologies in clinical trials;
- Bolsters federal pandemic preparedness and response efforts and invests in the public health workforce; and
- Improves cybersecurity of medical devices and cosmetics and personal care product safety.
Notably, the Act neither fulfilled the Biden Administration’s request for additional COVID-19 response funding nor included the Verifying Accurate Leading-edge In Vitro Clinical Test (IVCT) Development (VALID) Act, which proposed updating the current diagnostic testing regulatory framework. The Act also did not provide the Department of Labor enforcement authority (which was requested in its 2022 Report to Congress) to issue civil monetary penalties against health plans that it finds are noncompliant with the Mental Health Parity and Addiction Equity Act (MHPAEA). We expect issues regarding regulation of diagnostic tests and mental health parity enforcement to resurface in the new Congress.
Starting in 2023, the Administration will promulgate regulations to implement the Act’s provisions and to issue reports to Congress as required by statute, including on telehealth utilization, the Acute Hospital Care At Home program, pandemic preparedness efforts, and clinical trials reform, among others. We anticipate that there will be opportunities, via the federal rulemaking process, to address issues that were not included in the Act. The 118thCongress will provide an opportunity for House Republicans to advance their legislative and oversight agenda, namely the House GOP Healthy Future Task Force. With changing leadership of the Senate Health, Education, Labor and Pensions and House Ways and Means committees, new leaders will continue to conduct oversight responsibilities and pursue their respective health care legislative agendas. While the divided Congress will prevent significant legislative overhauls over the next two years, there will be additional opportunities for policy changes through must-pass legislation and reauthorization of programs that may receive bipartisan consensus. For more information, or to better understand how the Act impacts your organization, please contact the professionals listed below, or your regular Crowell & Moring contact.
Health Care Provisions included in the Consolidated Appropriations Act, 2023
The following sections outline the Act’s health care provisions and accompanying explanatory report and provide funding levels for Department of Health and Human Services (HHS) agencies. Legislative text and the Labor, Health and Human Services, Education, and Related Agencies summary and explanatory statement are included. The explanatory statement clarifies Congressional intent and directs the submission of a report to Congress.
Telehealth
Section 4113 of the Act extends certain Medicare telehealth flexibilities that were allowed during the COVID-19 PHE for two years, through 2024. The section waives the following telehealth services under Medicare: removes geographic and originating site requirements (through December 31, 2024); expands the list of practitioners eligible to furnish telehealth services (through December 31, 2024); extends telehealth services for Federally Qualified Health Centers and Rural Health Clinics (through December 31, 2024); delays in-person requirements for telemental health services (through January 1, 2025); and allows the furnishing of audio-only telehealth services (through December 31, 2024).
In response to the outbreak of the COVID-19 virus, Congress passed the Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020 and the Coronavirus Aid, Relief, and Economic Security Act (CARES Act), which gave HHS the authority to waive certain Medicare restrictions regarding coverage and payment for telehealth services during the COVID-19 PHE. Congress took additional action through the Consolidated Appropriations Act, 2022 to temporarily extend these flexibilities for 151 days after the end of the PHE. The PHE, which HHS Secretary Becerra renewed for the 11thtime on January 11, remains in effect through mid-April 2023. It is unclear whether the PHE will be extended beyond April. The section ensures that telehealth flexibilities under Medicare are extended for two years, regardless of the status of the PHE.
Section 4113 also requires HHS to conduct a study on program integrity related to telehealth services under Medicare Part B, including to review telehealth’s impact on future utilization of health care services (i.e., hospitalizations and emergency department visits) and to audit Medicare claims to assess potential fraud. HHS is directed to submit to Congressional committees the result of findings in an interim report in October 2024 and a final report in August 2026.
Acute Care Hospital at Home Program and Rural Health
Section 4140 of the Act extends the Acute Hospital Care at Home program for two years, through December 31, 2024. In November 2020, the Centers for Medicare & Medicaid Services (CMS) announced the Acute Hospital Care At Home program to provide hospitals expanded regulatory flexibility and allow them to care for eligible patients in their homes. As outlined in Section 4140, hospitals participating in the program must apply for a waiver and adhere to screening and patient safety standards. Section 4140 also requires the HHS Secretary to conduct evaluate quality of care and clinical conditions of patients in comparison to traditional inpatient care delivery, cost and quantity of services, and socioeconomic information of beneficiaries treated under the program. HHS must post the findings of its study on CMS’ website by September 30, 2024. In addition, Section 4137 of the Act extends, for one year through December 31, 2023, the 1% add-on payment provided to certain home health agencies that provide services in rural communities.
Medicare Payment
The Act makes numerous Medicare payment policy changes. Section 4111 of the Act extends incentive payments for alternative payment models for an additional year to calendar year 2025, at 3.5% as opposed to the current 5%. Section 4112 of the Act provides partial relief from 2023 Medicare Physician Fee Schedule reimbursement rates, which would have imposed a 4.5% reduction in 2023. The section reduces the cut to 2% for 2023 and 3.5% for 2024.
The Act makes several changes to “sequestration” (the automatic reduction of certain federal spending by a uniform percentage) of the Medicare program. Section 1001 of the Act delays the 4% Statutory Pay-As-You-Go Act of 2010 (PAYGO) sequester for two years, through the end of calendar year 2024. Under PAYGO requirements, Congress must pay for legislation by reducing entitlement spending or increasing revenue. Triggered by enactment of the American Rescue Plan Act of 2021, the 4% cut to the Medicare program would have taken effect in January 2023. The Act’s health care offset title includes Section 4163, which extends the 2% Budget Control Act of 2011 Medicare sequester for six months into FY 2032 and lowers the payment reduction percentages in FYs 2030 and 2031.
Mental Health: Medicare Coverage, Provider Assistance, and Parity Implementation
The Act provides funding for several programs addressing mental illness, substance use disorder, and crisis response, including community mental health services block grants and specific programs for pediatric, maternal, and veterans’ mental health. Section 4121 of the Act adds coverage for intensive outpatient programs and services furnished by marriage and family therapists and mental health counselors under Medicare Part B. Section 4126 of the Act adds a new exception to the Stark Law to allow for hospitals and other entities to provide evidence-based programs for physicians to improve their mental health, increase resiliency, and prevent suicide among physicians.
The Act also contains provisions eliminating the opt-out for non-federal governmental health plans for mental health parity requirements and ensuring compliance with mental health and substance use parity requirements. While MHPAEA established federal parity requirements for group health plans and health insurance issuers to provide mental health or substance use disorder benefits, it allowed state and local government employer-sponsored group health plans to opt out of compliance. Section 1321 of the Act eliminates the election option and requires self-funded, non-federal governmental health plans to comply with MHPAEA requirements beginning 180 days after the Act’s enactment. In addition, Section 1331 of the Act authorizes grants to states to enforce and ensure compliance with mental health and substance use disorder parity requirements.
Provider Directories
The Act also requires updates to Medicaid policies for mental health, including Section 5123, which requires a searchable directory of providers and guidance from CMS on access to crisis response networks under Medicaid. Effective in July 2025, Section 5123 codifies requirements that apply to Medicaid managed care organizations, prepaid inpatient health plans, and primary care case management entities regarding the publication of searchable and regularly updated directories of health care providers in their networks, including mental health and substance use providers. These requirements would also apply to state Medicaid fee-for-service programs.
Medicaid and CHIP Coverage
Section 5131 of the Act provides funding and establishes requirements for state Medicaid programs to support the transition from the enhanced Medicaid funding and continuous coverage requirements of the Families First Coronavirus Response Act (FFCRA). The FFCRA authorized increased federal funding to states through a 6.2 percentage point increase in Medicaid matching rates, or federal medical assistance percentage (FMAP), in response to the COVID-19 PHE. Section 5131 sunsets FFCRA’s continuous coverage requirement as of April 1, 2023 and allow for states to begin the process of initiating redeterminations of eligibility over a period of at least twelve months. States would be able to receive enhanced Medicaid funding from April 1 through December 31, 2023, subject to meeting certain conditions and at gradually reduced percentages. The enhanced FMAP will fully sunset by January 2024.
The Act also provides investments in Medicaid and the Children’s Health Insurance Program (CHIP). Section 5112 of the Act requires children to be provided with 12 months of continuous coverage in Medicaid and CHIP effective January 1, 2024. Section 5113 of the Act makes permanent a state option (provided by the American Rescue Plan Act) to allow states to continue to provide 12 months of continuous coverage during the postpartum period in Medicaid or CHIP. The American Rescue Plan Act allowed states to provide 12 months (rather than the required 60 days) of continuous postpartum coverage, but the authority was only available for five years.
Clinical Trials Diversity and Modernization
The Act includes numerous provisions to improve diversity among clinical trial participants and to modernize clinical trials, including through advancing decentralized clinical trials. Section 3602 of the Act requires FDA to issue new guidance or update existing guidance specifying the form and content of diversity action plans for enrollment, disaggregated by age, group, sex, and racial and ethnic demographic characteristics of clinically relevant populations. Section 3602 also requires sponsors to outline diversity goals, including demographic-specific outreach and enrollment strategies, study-site selection, clinical study inclusion and exclusion practices, and any diversity training for study personnel. Section 3603 of the Act requires FDA, in consultation with drug sponsors, medical device manufacturers, patients, and other stakeholders, to convene public workshops to solicit input from stakeholders on increasing the enrollment of historically underrepresented populations in clinical studies within a year of the Act’s enactment. Section 3604 of the Act requires FDA to issue a report on an annual basis, beginning two years after the Act’s enactment, that summarizes its diversity action plans.
Section 3606 of the Act requires FDA to issue draft guidance that addresses considerations for decentralized clinical studies, including the engagement, enrollment, and retention of a meaningfully diverse clinical population with respect to race, ethnicity, age, sex, and geographic location. The guidance must address recommendations related to advance digital health technologies (e.g., telehealth) that could support decentralized clinical trials, improve subject recruitment, retention, and engagement, and encourage meaningful diversity among clinical trial participants, including with respect to race, ethnicity, age, sex, and geographic location, as appropriate. FDA is required to finalize this guidance no later than one year after the public comment for the draft guidance ends.
Section 3607 of the Act requires FDA to issue guidance to modernize and improve clinical trials, including on digital health technologies in clinical trials to help improve recruitment, participation, and data collection and on innovative clinical trial designs to support the expedited development and review of drugs and biological products. FDA is required to finalize the three guidance 18 months after the public comment for the draft guidance ends. The section also requires FDA to work with foreign regulators with respect to the use of digital health technologies in clinical trials, decentralized clinical trials, seamless, concurrent, and other innovative clinical trial designs.
Pandemic Preparedness
Section 2101 of the Act requires Senate confirmation of the Director of the Centers for Disease Control and Prevention (CDC) beginning on January 20, 2025, and establishes specific functions of the Director. It also requires an agency-wide strategic plan to be developed every four years that describes CDC’s priorities and objectives, the capabilities that need to be developed to achieve these objectives, and how CDC will leverage strategic communications, external partnerships, and coordination with other agencies.
Section 2103 of the Act provides additional authority for HHS to coordinate with other departments and agencies in leading the federal public health and medical response to a public health emergency and includes a Government Accountability Office (GAO) study on the use of existing authorities for related interagency agreements. It also clarifies the role and responsibilities of the Assistant Secretary for Preparedness and Response (ASPR) in public health and medical preparedness and response activities. The section requires national- and state-level full-scale exercises every five years to identify and address gaps in preparedness and response, including the ability of the Strategic National Stockpile to appropriately support the response to a large-scale, long-term public health emergency. The section also requires HHS to submit an annual report to Congress on the state of public health preparedness.
Sections 2221 to 2227 of the Act provide funding to revitalize the public health workforce, including providing loan forgiveness to public health workers through reauthorizing the Public Health Workforce Loan Repayment Program, directing funds to recruit and train community health workers, and increasing educational opportunities for allied health professionals from underrepresented backgrounds.
Medical Device Cybersecurity and Cosmetics Reform
Section 3305 of the Act requires medical device manufacturers to ensure that their devices meet certain minimum cybersecurity standards. Effective 90 days after the Act’s enactment, these requirements include submitting a plan to FDA to monitor, identify, and address post-market cybersecurity vulnerabilities and exploits, including coordinated vulnerability disclosure and related procedures. The section requires manufacturers to ensure that devices and associated systems are secure and to release post-market software and firmware updates and patches as necessary. It also requires FDA to provide additional resources and information about improving cybersecurity of devices within 180 days, and GAO to issue a report, within one year, identifying challenges in this space and how federal agencies can strengthen coordination to improve in cybersecurity for devices.
The Act also expands FDA authority to regulate the safety of cosmetics and personal care products. Sections 3501 to 3508 of the Act direct FDA to establish good manufacturing practices, require cosmetic manufacturers to register their facilities and report adverse events, require cosmetic product labels to list fragrance allergens and contact information to report adverse event reports, and provide FDA with mandatory recall authority for cosmetics.
Health Care Provisions included in the Labor, Health and Human Services, Education, and Related Agencies Explanatory Statement
Artificial Intelligence (AI) and Machine Learning
The explanatory statement highlights efforts by the NIH and clarifies Congressional intent to direct agencies to build machine learning capacity and accelerate the pace of biomedical innovation. It expresses strong support for NIH's efforts to build AI-based analytical tools to help NIH optimize investments in biomedical research by identifying emerging topics and predicting which ones will produce transformative breakthroughs.
In addition, the explanatory statement includes language that requires ASPR to issue a report to Congressional committees, within 120 days of the Act’s enactment, on the feasibility of creating an AI-enabled Pandemic Preparedness and Response Program. The program would adopt AI programs to shield the nation against current and future bio-threats and use AI to develop accelerated vaccines, rapid therapeutics, global bio-threat surveillance, and rapid fielding.
340B Drug Pricing Program
The explanatory statement also includes language directing HRSA to provide a briefing to Congress, within 120 days of the Act’s enactment, on actions taken to safeguard 340B covered entities’ lawful access to discounted drugs.
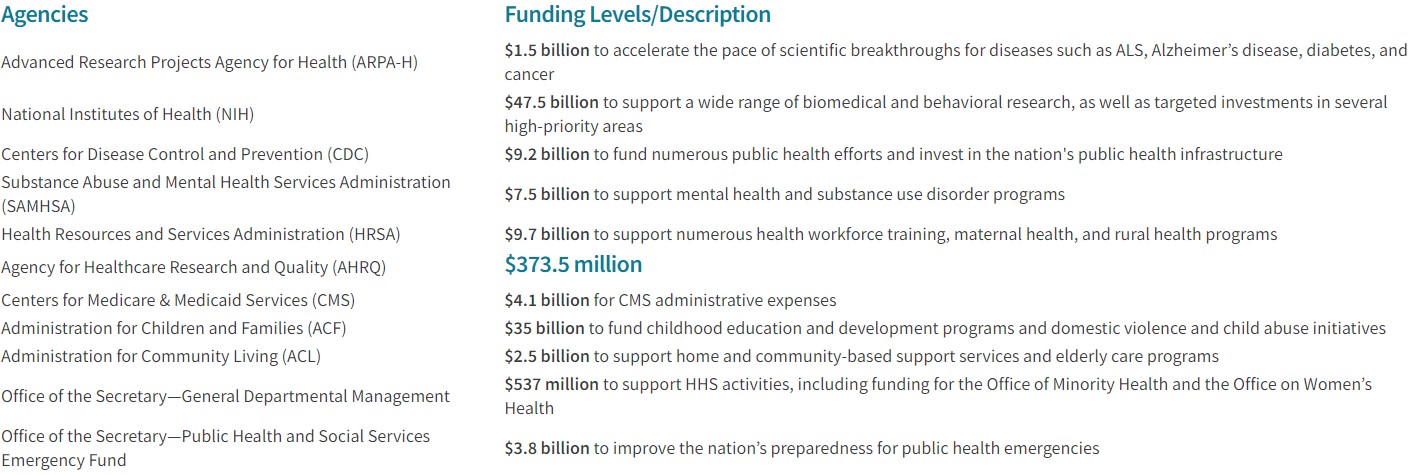
FY 2023 HHS Funding Levels
The Act provides a total of $120.7 billion for HHS, an increase of $9.9 billion above the FY 2022 enacted level, including the below funding levels for agencies.
Insights

Client Alert | 3 min read | 08.03.26
On July 20, 2026, New Jersey Governor Mikie Sherrill signed the Forbidding the Algorithmic Inflation of Rent (FAIR) Act into law, making New Jersey the fourth state to regulate algorithmic rent-setting practices. Three days later, on July 23, 2026, Governor Sherrill signed the Fair Price Protection Act, which targets “surveillance pricing”—the practice of using or collecting personal data about a user and using an algorithm or artificial intelligence to charge different consumers different prices for the same products. Together, these laws represent a significant expansion of New Jersey's consumer protection framework in the algorithmic pricing context.
Client Alert | 2 min read | 08.03.26
New York Becomes First State to Restrict Addictive Social Media Features for Minors
Client Alert | 4 min read | 08.03.26
Client Alert | 6 min read | 08.03.26
The Pipe, Not the Posts: How Section 230’s Protections Extend to Generative AI Platforms